A little over a year ago, a professor at a prestigious
nursing school reached out to me via my website asking if I’d be
interested in writing the infertility chapter in a women’s health nursing textbook.
I was flattered and realized it would be an amazing opportunity.
I was also a little nervous.
I weighed the risks and benefits. Writing a chapter in a
textbook would be an amazing accomplishment, ensuring that I am up to date with
my knowledge of reproductive endocrinology and infertility (REI) while also
lending credibility to me as an ‘expert’ in my field. Also, the timing was good.
I recently broke my foot and was frustrated that I was unable to run or exercise,
so tackling a project like this would be a good distraction.
It would be a big undertaking, though. I’d written articles
for journals, blogs, and websites, but the last time I contributed to a book
was when I wrote a chapter of questions for a study guide. I was hesitant to
re-enter the academic arena, as I became disenchanted with writing for academic
publications after enduring an arduous editing process for an article that I
wrote on polycystic ovarian syndrome (PCOS).
Did I want to write a whole chapter?
After making a pro-con list and receiving advice from a few
trusted friends, I ultimately went with my gut and emailed the editor accepting
the assignment.
I met my deadlines and was even ahead of schedule to send in
my first draft, but as I prepared to email it, I had a mini panic attack: What if
any of my content is out of date? What if someone used my information and the
resulting patient care was subpar? Who did I think I was, writing a chapter
that was going to be used in prestigious nursing schools?
Hard at work while elevating my foot
I spun into a full-blown shame spiral. This wasn’t the first time I felt like I
didn’t earn my spot, or that I was a fraud, a phenomenon that I knew well and
later realized was called ‘Imposter Syndrome’.
My first recollection of it was when I was a teenager. I started
piano lessons when I was 6, and every year there was a recital. Each student
would climb up on a big stage and play his/her memorized piece to the large
group of friends and family members assembled there. The recital, like many performances,
started with basic pieces and ended with more complex, challenging ones. The message
was that the last few performances were worth waiting for. At 16 years old (after
10 years of lessons) I made it to the next-to-last-spot for the recital that
year (the ‘closer’ was a 12-year-old prodigy who, I reassured myself, was probably
not as well-rounded as me).
When my name was announced, I, in all of my adolescent awkwardness, took my spot at the piano, sweating in an uncomfortable dress and hobbling on high heels that my mom forced me to wear, and sat on the bench. I placed my hands over the keys and my feet over the pedals, took a deep breath and…froze. Froze like in a comedy movie or a nightmare. My thinking brain sounded the alarm: What the hell was I doing? I didn’t belong there! I had been faking it all along! Wait until everyone realizes that I really can’t play.
Somehow, through sheer force of will, I finished, but that moment of panic and self-doubt led to the end of my music lessons and performances. In fact, I didn’t play the piano again until I was well into my 40’s.
The day that the first draft was due brought me back to that stage, and the accomplished adult that I now was regressed to that awkward adolescent girl in the starchy dress and ill-fitting pumps with performance anxiety.
Who did I think I was?
Was my work worth waiting for? How could I allow myself to be vulnerable like this?
Vulnerability as a positive quality is getting a lot of well-deserved traction in the media and academic circles, largely due to the work of Dr. Brene Brown who described it as ‘… not winning or losing; It’s having the courage to show up and be seen when we have no control over the outcome. Vulnerability is not weakness, it’s our greatest measure of courage’. I personally feel so strongly about the value of vulnerability as a clinical provider that I discuss it in almost all my learning modules and presentations.
I now had an important decision to make: Will I have the
courage to practice what I preach?
I heard once that being brave is not accomplished solely in the
form grand gestures or sentinel events. It is grown and cultivated in small
moments like this, and something in me changed that day. I decided, at that
moment, that I was no longer going to be ruled by shame nor defined by my
imperfections. I resolved, at that moment, to allow myself to be vulnerable and
put my work out there, even if it gets criticized. I came to the conclusion
that striving to be perfect no longer serves me.
With this in mind, I hit ‘send’.
Ultimately, the book was published, and a copy was sent to me. I’d be lying if I didn’t admit that I was a little giddy receiving it and seeing my name in print. Although I can’t count the number of hours I spent writing and revising it, I don’t regret the time spent. I crafted and molded it until it had the right tone. I researched the shit out of it until I was confident that even if I missed something, I did the best that I could. It became something of which I was proud, and I felt justified being the person who was meant to write it.
‘It is impossible to have lived without failing at something, unless you live so cautiously that you might as well have not lived at all-In which case you fail by default.’
J.K. Rowling
I realize that, like the textbook, our lives have chapters. I
am done with the one where I doubt myself and my abilities.
Maybe the accomplishment, in this case, is not in writing a
chapter, but in closing one.
It’s amazing how a single image can generate two polarized feelings. This one triggers, in me, both intense joy and unbelievable loss. It was taken at a conference about two months after I found out I was pregnant.
I remember my husband and I seeing the heartbeat on ultrasound, the only appointment that he was able to make, and us laughing and conspiring about how I was going to keep my pregnancy a secret at the conference. I worked in women’s health, was well-versed in pregnancy loss and, as a result, we decided that we wouldn’t tell anyone until we were out of the first trimester. I had bought a new dress for the speaker dinner (the one in this picture) and we laughed at the waste of money as I probably wasn’t going to fit into it by then. How was I going to explain why I wasn’t drinking without revealing that I was pregnant to a roomful of woman’s health specialists who can sniff out a pregnant woman a mile away?
Well, I was able to wear my new dress and drink my white wine because I lost the pregnancy.
On the day that I found out, I watched as my OB/GYN’s expression changed from happy curiosity to confusion and then despair as he futilely searched for the baby’s heartbeat at the ultrasound appointment that I had (idiotically) scheduled on my birthday. I almost felt worse for him than I felt for myself, when he had to tell me that the baby had stopped growing, the pregnancy was essentially lost, and then offered me medical or surgical ‘options’. I chose to have a D & C because my boss at the infertility office where I worked had a planned vacation and was leaving for a week, a week in which I would help cover the office by performing ultrasounds on patients who were pregnant. Imagine that: Performing pregnancy ultrasounds on patients after having just experienced your own pregnancy loss.
I read once that being emotionally brave isn’t a gift or something that you born with, it’s something that you work toward in small increments.
I wanted to be ‘brave’ but I didn’t really know what that meant in this case. I know what NOT to say when someone has a loss, hell I teach nurses how to have difficult conversations with people as part of my nursing education business! But when it’s happening to you, particularly when you don’t have the time or space to grieve, you feel stuck. All of the knowledge that I had on how to handle grief became unraveled by the physical and emotional pain that a pregnancy loss can generate. I read once that being emotionally brave isn’t a gift or inherited trait, it’s something that you work toward in small increments. It’s forcing yourself out of your comfort zone and doing brave little things on a regular basis until the pit in your stomach lessons or subsides, until your breathing is less shallow or your throat less tight.
I made it through that week with the help of close friends and my husband. I had to suppress my grief, short-term, in order to function as a clinician in an office of patients who needed me, but the evenings that week were incredibly tough, as were the following months when unacknowledged grief would rear it’s ugly head in the form of an unkind word that I would say or my desire to stay in bed on a beautiful Spring day. Most people don’t understand the depth of a loss like this. My sweet boss came back and, upon finding out about my pregnancy loss and subsequent need to cover the office in his absence, asked “Was that tough for you?” Uh, yeah, and thinking only a dude would ask that?!?
Emotions are simply energy that is flowing through your body at that moment, and they can either pass through or get stuck.
Once time passed and somewhat tempered my feelings of loss and inadequacy, I was able to find a sliver of gratefulness as a result of this experience. I gained a true understanding of grief, and how you need to lean into it and go through it to get to the other side. Even though it seems like strong feelings can hurt you, they can’t. Emotions are simply energy that is flowing through your body at that moment, and they can either pass through or get stuck. How long they take to pass and their level of intensity can differ, but I knew I had to allow them because I didn’t want to be stuck.
I’m not sure why we live in a world where being stoic in the face of grief is defined as brave. Why is crying, when you are sad, bad? You can’t escape or postpone pain, it will find it’s way out, so better to let yourself feel what you are feeling in that moment and many moments to come. Emotional suppression is not only overrated, it’s harmful. I find the work by Dr. Brene Brown on shame and vulnerability so compelling and truly feel that being brave is allowing yourself to be vulnerable. Importantly for us, as caregivers, it’s asking for help and allowing ourselves to be supported, in whatever form that takes. I share this personal story as part of my own journey toward vulnerability and in the hope of providing some perspective on pregnancy loss for those who have had it or those who know someone who has.
As an infertility nurse practitioner, I am asked this question often and it’s a valid one.
First, I want to say that I am so sorry. I understand how devastating this news is. By explaining the potential reasons why this treatment cycle didn’t result in a pregnancy I don’t mean, in any way, to diminish the sadness and frustration that you might be having, only to give you information that, in my experience, many people desire in your situation.
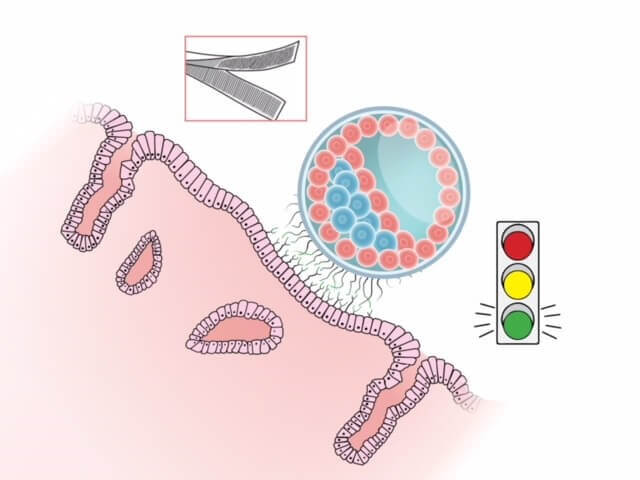
Let’s discuss what preimplantation genetic testing (PGT) is and does. An embryologist gently removes a few cells from the early placental portion of a blastocyst (a day 5-6 embryo that has hundreds of cells at this point), extracts the DNA and sends them to a special lab to be analyzed for the number of chromosomes. Humans have 23 chromosomes but get a copy of each one from both parents. Normal embryos are called euploid and contain 46XX if female or 46XY if male. Abnormal embryos, called aneuploid, would not have this normal complement of chromosomes. Any of the 23 human chromosomes can be abnormal in different ways and have one too many (called a trisomy) or one too few (called a monosomy). Some chromosomes are more commonly abnormal than others, but they can all commonly and randomly be abnormal in embryos. Aneuploidy is the by far the most common reason for miscarriages in humans. PGT allows us to identify these aneuploid, or abnormal, embryos before any are transferred back into your uterus. Since the most common reason for recurrent implantation failure and miscarriage in women >38 y/o is aneuploidy, the ability to use PGS prior to embryo transfer has improved clinical pregnancy rates tremendously in this age group.
It is completely normal that a percentage of every women’s eggs, and therefore embryos, will have chromosomal abnormalities, but the proportion of normal embryos goes down with age, and that of abnormal embryos goes up with age. Women with diminished ovarian reserve/egg quality may have a higher percentage that are abnormal, compared to women with normal ovarian reserve of similar ages.
Let’s assume that out of all the blastocysts analyzed in your cycle, there are some that were euploid (or had the normal number of chromosomes). Your reproductive endocrinologist (RE) transferred one of these into your ‘optimally primed’ uterus, supported by ‘perfect’ hormone levels. You behaved yourself, rested for a bit after transfer, didn’t sneeze too hard, stopped going to spin classes and didn’t drink your evening glass of wine. Now, it’s just waiting for implantation to occur. Why wouldn’t a pregnancy test be positive in this scenario?
Because implantation is a relationship. Like any relationship, there is an attraction, an investigation period, then, if all is a go, lots of energy and effort is required for it to continue. So, we have an embryo that should work (a person that ‘seems’ normal/’looks good on paper’) and a lining that should be receptive (both are ‘ready’ for a relationship). But, like every relationship, even with two strong prerequisites, there may not be a lasting connection or the timing may be ‘off’.
Although our technology has improved greatly over the last 5-10 years, and our diagnostic testing continues to be refined, even with ‘normal’ results, we can’t predict that that person will have a clinical pregnancy. For example, a normal semen analysis result tells us that there is enough motile sperm to fertilize an egg, but the real test is if fertilization takes place. The saline sonogram or hysterosalpingogram tells us that the uterus ‘should’ be able to carry a pregnancy. PGT testing tells us that we have a normal embryo that ‘should’ create a baby. On paper, we have all the building blocks necessary for a successful pregnancy.
But people aren’t pieces of paper. We are infinitely more complex and nuanced. There are important dynamics necessary for implantation that we are just learning to identify and can’t treat (yet) if they are lacking or abnormal.
Implantation is just the first step in a cascade of interrelated events necessary for a clinical pregnancy to take place. Earlier, we discussed chromosomes and genes. Although important concepts, when discussing them, we are only describing what happens in the nucleus of the cell. The other part of the cell (the body of the cell, if the nucleus is the brain, per se) is called the cytoplasm, and it is also important for cell division and reproduction. In the cytoplasm are many organelles, structures important for the functioning of that cell. For example, the mitochondria are located here, and they are responsible for providing the energy necessary for all of the processes for that cell. When the cell ages, the cytoplasm and the mitochondria age too. So, even though an embryo is euploid, the mitochondria may be suboptimal and not produce enough energy to fuel blastocyst development and differentiation. Early embryo development and differentiation are hard work (actually some of the most energy-requiring processes in the entire body). When the energy-producer (mitochondria) can’t meet this need, these processes themselves can suffer, which can lead to early pregnancy loss or failure to implant and grow.
Although this article is mostly about the embryo component of implantation, as we are well-aware there is a uterine component too. How do we determine that a woman’s uterine lining is receptive? The testing that we used to use (such as an ultrasound or endometrial biopsy where the cells are reviewed microscopically by a pathologist) has been shown to have poor predictive value. There is emerging research, though, that utilizes DNA analysis to reveal patterns that were too subtle to see using previous technology. These investigators can, then, attempt to pinpoint that particular woman’s window of implantation (as opposed to assuming that every woman has the same window). This technology, and others like it, is promising, but we still have much work to do to discover and improve the propensity for the embryo to attach to the uterine lining, or to help the body find the right ‘fit’ between the best embryo and the ideal spot in the uterus in which it should implant.
Does this mean that since the first cycle didn’t result in a healthy pregnancy, that subsequent cycles won’t either? The short answer is no. In my experience, there are many who do not get pregnant on their first try with PGT but do get pregnant on future cycles with a different euploid blastocyst. So even though the building blocks of a healthy pregnancy were present for both cycles, we don’t have an answer for why only the second one worked. Yet.
For some, having the facts can help them accept the current situation and maybe lessen any guilt or other negative emotions generated as a result of an unsuccessful treatment cycle, however we realize that information doesn’t detract from the pain or lesson the emotional toll that a failed cycle can trigger. We encourage you to continue your journey as you see fit and want to acknowledge how brave and resilient you already have been and will continue to be. How do we know this? Because we, as nurses, are witness to your courage and tenacity every day; because you are reading this blog; because you are asking questions; because you are making informed, rational decisions about a situation that is anything but rational, at times.
Because you are not allowing yourself to be hobbled by a difficult journey. That is true strength.
The fact that someone else loves you doesn’t rescue you from the project of loving yourself
Sahaj Kohli.
A final thought: please offer yourself all the compassion and tenderness that you can muster during this vulnerable time.
Many of us don’t realize how well the intricate system of feedback loops in our reproductive endocrine system work until they are disrupted in some way. Polycystic ovarian syndrome (PCOS) represents an example of this. It is a disorder characterized by a collection of symptoms, and is prevalent in patients who present at infertility clinics, affecting 5-10% of women at reproductive age. An estimated 90% of anovulatory cases are related to PCOS. In addition to negatively affecting metabolic parameters and ovulation, it is also associated with several mental health issues (such as depression and anxiety) in the women who have it. It is, though, manageable by using medical and non-medical interventions. It is beyond the scope of this article to fully explain PCOS, so in part 1, we will discuss the pathophysiology of PCOS, its diagnostic criteria, insulin and leptin resistance, psychological implications and the clinician’s unique role in supporting the patient with PCOS.
Pathophysiology of PCOS
In ovulatory women, under the influence of a properly functioning hypothalamic-pituitary-ovarian (HPO) axis, the menstrual cycle is characterized by the growth and development of (usually) a single follicle that is extracted from that month’s cohort (group of follicles). In response to GnRH stimulation, the anterior pituitary gland secretes two important gonadotropins: Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH). FSH acts on the ovary to help grow and mature small follicles. That month’s dominant follicle is one which has acquired the most FSH receptors. This follicle will continue to grow and mature at the expense of the remaining small follicles, which then get reabsorbed by the body (but are still deducted from the woman’s total egg supply). Growth of the dominant follicle generates estradiol production and elevated estrogen levels signal FSH production to cease via a negative feedback system, but a high and sustained estrogen level will trigger a one-time surge of LH which causes ovulation to occur.
In a woman with PCOS the HPO axis does not express normal functionality. The pulsatile hormone GnRH is altered, resulting in increased LH activity by the pituitary gland. This increase in LH increases theca cell stimulation (see Fig 1), which produces androstenedione and testosterone, two androgens, and the resulting hyperandrogenic milieu of the ovary precludes normal follicular growth, maturation and ovulation. The ovary, then, becomes comprised of many small, antral follicles that never become dominant. The collection of these follicles can cause an increase in the size of the ovaries and generate a slightly elevated basal serum estrogen level. It remains unknown why PCOS occurs and whom it affects, but it is thought that genetics and environmental factors have a complex interplay in its emergence and clinical manifestations.
Fig 1: There are two cells in the ovary that contribute to estrogen production and they work synergistically. The theca cell converts cholesterol to two androgens (androstenedione and testosterone) under the influence of LH. These androgens then travel through the basement membrane into the granulosa cell which, under the influence of FSH, converts them to estrogen via a process called aromatization. Excess LH stimulation, then, will generate more androgens than can be converted to estrogen, so the estrogen level never becomes elevated enough to generate an LH surge and the ovary has a hyperandrogenic milieu.
Diagnostic Criteria
PCOS is not defined or diagnosed by one simple symptom and is often a diagnosis of exclusion for women who have oligo-ovulation and evidence of hyperandrogenism(such as acne alopecia and hirsutism (male-pattern hair growth and texture) once other disorders are excluded. It affects women of all shapes, sizes, and backgrounds.Although symptoms can start at menarche, most clinicians are reluctant to diagnose arelatively newly menstruating adolescent with PCOS as menstrual cycle irregularity is normal in the first yearpost menarche and can resolve in time.The diagnostic criteria most commonly usedtoday were revised in an international expert workshop in Rotterdam, The Netherlands,in 2003 and are called The Rotterdam Criteria wherethe following were established: PCOS can only be diagnosed when a patient has at least two out of three features: oligo/anovulation, hyperandrogenism (biochemical or clinical), and the appearance of polycystic ovaries upon ultrasound. Hyperandrogenism is diagnosed either clinically (by the clinician observing androgenic symptoms) or biochemically (such as elevatedserum free testosterone levels).
Other conditions that can cause irregular menstrual cycles (pregnancy, hypo– and hyperthyroidism, ovarian failure and hyperprolactinemia) and hyperandrogenism (congenital adrenal hyperplasia, adrenal tumor and androgen–secreting tumor) must be ruled out first, so in addition to serum bHCG levels, basal FSH and LH levels,thyroid stimulating hormone (TSH), prolactin, total and free testosterone, 17 hydroxyprogesterone(17OHP),dehydroepiandrosterone sulfate (DHEAS) are drawn.One of the most difficult differential diagnoses is discerning a woman withfunctional hypothalamic amenorrhea(FHA) versus a lean woman with PCOS. Classically women with FHA have a low BMI, but it also can be in the low/normal range. Both conditions are characterized by anovulation and ovaries which appear to have many small follicles in a resting state. Whilehyperandrogenism is not a component of FHA, women with the condition may have hirsutism due to their ethnicity, further confusing the clinical picture. One way to distinguish FHA from PCOS is with blood testing and ultrasound examination. Women with FHA often have low to normal basal FSH and LH levels (due to hypo–stimulation of the ovaries) and a low estrogen level whereas women with PCOS typically have elevated serum LH levels and low to normal FSH levels. On ultrasound, the uterus and ovaries of women with FHA are small or small/normal, whereas women with PCOS typically have an increased ovarian volume (>10 ml).There is emerging research on a possible connection between both FHA and PCOS as not all women present with characteristic features of either condition andFHA and PCOS do have some overlapping characteristics.
Insulin Resistance and Leptin Resistance
Although the diagnosis of insulin resistance (IR) is not part of the Rotterdam Criteria,it is incredibly prevalent in women with PCOS. An elevated BMI increases the chance that a woman with PCOS has IR, but evennon-obese women with PCOS are far more likely than their size-matched counterparts without PCOS to develop insulin resistance. In addition to the health consequences of IR (such as metabolic syndrome and type 2 diabetes mellitus), it also exacerbates and contributes to hyperandrogenism in a patient population who is already suffering from it.
The gold standard for diagnosing insulin resistance is to use a hyperinsulinemic euglycemic clamp, a test which must be performed in a hospital setting. To most, this is unreasonable, so indirect testing for IR is done. In women with PCOS in a preconception clinical setting, the suggestion is to do perform an oral glucose tolerance test (OGTT)given the high risk of women with PCOS to develop impaired glucose tolerance and gestational diabetes in pregnancy. Although somewhat time-consuming, this test is preferred over fasting plasma glucose and insulin levels alone as it can diagnose impaired glucose tolerance at an earlier stage. In women with PCOS who are not in a high-risk category (i.e., BMI<25 kg/m2, not trying to conceive, no personal or family history of impaired glucose tolerance)obtaining at least baseline fasting glucose, insulin and hemoglobin A1clevels can be helpful in order to get a ‘snapshot’ of that patient’s glycemic status.
….the conditions of overweight and obesity are common in women with PCOS and weight loss can feel impossible since intuitive eating is not effective when hunger and satiety cues are unreliable.
When a woman has PCOS, being overweight or obese intensifies the metabolic consequences. White fat cells are metabolically active. At a normal level, they are protective as they provide a safe home for lipids and keep fat out of organs.When there are too many fat cells, they can get overloaded and burst, releasing fatty acids into the bloodstream which can affect every organ. These fat cells get ‘stuck’ between the cells in organs and cause them to be stiff, damaged, less functional and cause chronic inflammation. It is not uncommon to diagnose ‘fatty liver’ in a woman with PCOS who is obese, as the liver is particularly vulnerable. In addition, an excess in adiposity can perpetuate existing hyperinsulinemia and insulin resistance by disrupting the delicate balance of cytokines and hormones produced by adipose tissue (see Figure 2), for example, decreasing the production of cytokines which increase insulin sensitivity, and increasing those which promote inflammation and insulin resistance. Excess insulin further contributes to abdominal adiposity and hyperandrogenism creating a vicious cycle in PCOS patients that can be difficult to overcome.
Figure 2: Increased adiposity, and the subsequent increase in fat cells, can perpetuate hyperinsulinemia and insulin resistance by disrupting the delicate balance of hormones produced by adipose tissue, such as decreasing the production of adiponectin, a cytokine which increases insulin sensitivity and increasing others which promote inflammation.
In addition to insulin resistance, patients with PCOS and obesity may also suffer from, what some term, leptin resistance. Some studies have shown that leptin levels are higher in obese PCOS patients compared to lean patients. Leptin is a protein produced by adipose tissue which regulates the body’s energy balance and appetite. When properly functioning, an increase in leptinsignals the brain to reduce a person’s appetite and a decrease in leptin does the opposite, it signals the brain to increase appetite to provide the fuel needed for energy. In many PCOS patients with obesity, however, this system is faulty and, despite increased leptin concentrations secondary to the increase in adipose tissue, the efficacy of leptin decreases, leading to leptin resistance. Leptin resistance is considered animportant risk factor for the pathogenesis of overweight and obesity, as the body remains insensitive to elevated levels and signals to the woman that she is still hungry/not satiated even after eating. Many women with PCOS complain of ‘never feeling full’ due to this resistance and continue to eat, leading to an increase in adipose tissue, which results in increased leptin resistance and perpetuates this damaging cycle. As a result,the conditions of overweight and obesity are common in women with PCOS and weight loss can feel impossible since intuitive eating is not effective when hunger and satiety cues are unreliable.
Education about the significance of having PCOS is vital and the main focus should be addressing the patient’s perceived needs while decreasing the long-term risk factors.
Figure 3: Disruption of the HPO axis in a PCOS patient. There is excess LH stimulation on the theca cell resultaing in an increase in testosterone levels, an androgenic ovarian environment, and anovulation (resulting in low progesterone levels). Increased leptin levels due to an excess of adipose cells affect GnRH secretion. Elevated insulin levels contribute to hyperandrogenism.
Impaired leptin secretion not only affects body weight but canhave a detrimental effect on ovulation (see Fig 3) and even fertilization in normal-weight PCOS patients. It alters the release ofGnRH from the hypothalamus, decreasing anterior pituitary stimulation (and therefore FSH and LH secretion), and preventing the development of a mature oocyte.In addition, the granulosa cells also store and produce leptin, and high levels of leptin decrease their aromatization capacity which ultimately interferes with the ability of a dominant follicle to produce adequate amounts of estrogen (see Fig 1).A small, observational study found a direct correlation between the concentration of leptin found in the follicular fluid (FF-leptin)(which has been correlated with fertilization rate) in lean women with PCOS who have underwent IVF when compared to normally ovulating, weight-matched women.
Managing PCOS
PCOS is not curable but is manageable with proper diagnosis and the patient’s understanding of (and dedication to) the life-long strategies that can ameliorate its consequences.Education about the significance of having PCOSis vital and themain focusshould be addressing the patient’s perceived needs while decreasing the long-term risk factors. Potentialmetabolic sequelae and dangerouscomorbiditiesassociated with a PCOS diagnosis includedyslipidemia, impaired glucose tolerance, visceral obesity and being susceptible to the development of diabetes andcardiovascular disease (CVD).Some research suggests that the PCOS condition, particularly when accompanied by obesity, is associated with chronic inflammation and oxidative stress which are hallmarks of cancer development.In fact,women with PCOS have an increased risk (2-6 fold) of endometrial cancer. There is also research suggesting that women with PCOS have higher incidences of autoimmune thyroid disease even in the absence of thyroid dysfunction symptoms. Women with PCOS may require more specific screening for this disease or screening at a younger age given their PCOS diagnosis.While the syndrome is nondiscriminatory, there is ethnic variation in the presentation and intensity of symptoms. For example, East Asian women appear less clinically affected by hirsutismand have a lower BMI than Caucasian women. Hispanic women incur a higher prevalence of metabolic syndrome and hypertriglyceridemia than other ethnic groups, and increased central adiposity, IR, diabetes and metabolic risks are found in South East Asians and Indigenous Australians.
One of the important goals of PCOS management is increasing the body’s sensitivity to insulin.Hyperinsulinemia, in addition to leading to insulin resistance, is a powerful contributor to excessive stimulation of ovarian androgens, and also inhibits sex hormone binding globulin (SHBG, a glycoprotein that helps to bind to androgens and reduces free testosterone levels which can improve hyperandrogenic symptoms).Lifestyle interventions are considered the first-line treatment for PCOS patients. Although weight loss ispreferable when a patient with PCOS is overweight or obese, some suggestthat the clinician emphasizes strategies that improve health as opposed to the focus solely being on weight loss. For example, exercise is the strongest insulin sensitizing strategy and is still helpful even in the absence of weight loss. Conversely, many PCOS patients are advised to lose weight prior to conceiving and they can do so in unhealthy and unsustainable ways, such as eating a no carb or extremely low-calorie diet, which might result in weight loss but can actually worsen metabolic parameters and is associated with high rates of recidivism.
Patients’ attitudes toward exercise can vary greatly and it is difficult for those living with obesity to engage in exercise or physical activity. They may feel physically unable, emotionally uncomfortable and/or apprehensive about being publicly embarrassed.
Patients’ attitudes toward exercise can vary greatly and it is difficult for those living with obesity to engage in exercise or physical activity. They may feel physically unable, emotionally uncomfortable and/or apprehensive about being publicly humiliated. Some patients in higher BMI categories might be embarrassed or reluctant to go to a gym or a group exercise class where they perceive that everyone is thinner or fitter than them and, until recently, it was difficult for plus-size patients to find attractive workout clothes. For this patient population, it might be helpful to encourage them start exercising with the use of home videos, find a trainer who is experienced in dealing with body-diverse clients, or find a body-positivity mentor in person or online. Beginners can work towards simple, non-scale-centric goals such as increasing their workout time from 30 to 45 minutes or being able to walk a mile, instead of relying on weight loss as the only outcome.
In addition to increasing insulin sensitivity, decreasing abdominal adiposityhas shown to be a successful treatment for both the hormonal and metabolic characteristics of PCOS and might restore ovulation and menstrual cycle regularity in some patients. Achieving “metabolic fitness” such as making improvements in lipid and glycemic status is also a reasonable goal. Adolescent women with PCOS, who are surrounded by images of thin, fit girls both in person, on social media, and in mainstream media on a regular basis, can find it difficult to make the mental shift from attempting to replicate a too-thin, unachievable body shape to feeling healthier and achieving a reasonable weight that is sustainable. There is no single diet that works for all clients with PCOS. Ideally, women with PCOS should meet with a nutritionist who has an endocrinology background and can create individual meal plans for based on food preferences, availability, budgetand other important factors. Proper nutrition counseling is a cornerstone in the treatment plans for PCOS patients.
The Psychological Consequences of PCOS
Although it is paramount to decrease or delay the onset of the long-term risks associated with PCOS, the patient’s focus might be on reducing or tempering its physical and emotional consequences. Unequivocally, PCOS canaffect a woman’s appearance which can negatively impact her self-esteem, particularly in adolescence. First, there is a high correlation between women with PCOS and elevated BMI. A reported 40-80% of women in this population are overweight or obese, often storing excess fat in the abdominal area. This form of adiposity called ‘visceral fat’ has a reciprocal relationship with hyperinsulinemia, where it is both exacerbated by, and contributes to,excess insulin.
The androgenic manifestations of PCOS can also be devastating. Women with the conditionoften present with hirsutism, moderate to severe acne and/or alopecia that is difficult to combat. Starting OCPs or other medications to reduce serum androgens will limit the progression of these and may help control acne, but they will not reduce the amount of current body hair, and scalp hair regrowth can be a long process. Since many women utilize electrolysis or laser hair removal (when they can afford to) to reduce the appearance of hirsutism,during the physical exam clinicians should ask about any hair removal methods in order to determine the extent ofclinician hyperandrogenism. The use of the FerrimanGallwey score(a visual scale that assesses hirsutism) can be helpful for documenting their baseline score (a score ≥ 4-6 indicates hirsutism depending on ethnicity), then noting any improvement subsequent to interventions. Excess androgens can also result in acne which can persist into the adult years. Consulting a dermatologist for acne and skin changes can help improve appearance.
This collection of symptoms can cause many PCOS patients to state that they do not “feel feminine” and, over time,often lead to depression or low self-esteem ultimately impacting their quality of life. Patients diagnosed with PCOS report increased psychological disturbances, and lower sexual satisfaction. Elevated BMI and hirsutism were the two highest reported features that contributed to decreased psychological well–being, while biochemical, endocrine and metabolic issues seem to be less urgent, an important distinction for counseling patients.
It is vital that the nurse recognizes the unique consequences of women with PCOS when working with this particularly vulnerable population. Many of these women have been victims of weight bias or prejudice, even in health care settings. They might feel imprisoned in a body that even they don’t understand, potentially mortified by their appearance at a pivotal time in their lives, and the brunt of jokes by classmates, officemates, even teachers and health care providers. Weight bias is pervasive, and people feel justified mocking those in higher BMI categories because they perceive that being overweight or obese is a choice and, therefore, under their control. So although women are taught that‘lifestyle changes’ can make a difference and ‘losing a small amount of weight is helpful’, this task seems daunting when their body craves foods that are caloric and fatty, and they do not achieve a feeling of fullness when they should. Weight bias has been shown to be incredibly detrimental to weight-diverse patients, and those who are victims of it feel frustrated and powerless leading tobinge eating and less exercise, the opposite of the desired outcome. In order to reduce bias, it would benefit the clinician to educate themselves on the complex reasons that people overeat prior to educating their PCOS patients.
Involve and empower the patient by asking her to identify her own goals, such as being able to run a race, feel comfortable in a group class with others…etc. During the medical history, clinicians can ask a question such as “What are some things you feel unable to do now that you would like to do” and then collaborate with her to make changes to accomplish these. Identifying short-term, achievable, concrete goals can embolden and encourage the patient and take the focus off weight loss, which has probably been attempted many times in the past. In fact, exercise is the greatest insulin-sensitizing strategy, regardless of weight loss.
To some, the diagnosis of PCOS is a relief as they now have justification for their androgenic symptoms and unexplained weight gain. For others, it is met with anger and resentment as it upends their version of adolescence or womanhood that they have probably had since childhood.
To some, the diagnosis of PCOS is a relief as they now have justification for their androgenic symptoms and unexplained weight gain. For others, it is met with anger and resentment as it upends their version of adolescence or womanhood that they have probably had since childhood. They are acutely aware that their bodies are different than those of their classmates and feel that they are not as attractive to potential partners. Control of their glucose levels and weightmight feel chaotic, resulting in a body that is as mystifying to them as it can be to others. Clinicians must realize thatacceptance of PCOS as a life-long disease can take years.
PCOS is a complex, multi-layered condition that is heterogenous in both its manifestations and its presentation. The physiology of these patients is distinct in that they have barriers to the protective feedback systems that maintain balance in the body, such as leptin and insulin, resulting in weight gain and hyperinsulinemia. Management of these patients is centered around sensitizing them to insulin, preferably utilizing non-pharmacological methods first. Having PCOS can create an emotional toll on a woman which must be considered by those who care for them, and education and interaction should be undertaken without biasor blame. The future of PCOS lies in researching the genetic and epigenetic etiologies of the disorder in order to refine the diagnosis and hopefully discover a cure. Patients should also be made aware of pharmacologic treatment strategies, and potential future reproductive options (which will be discussed in Part 2).
* The authors would like to thank Neil Chappell, MD for his help reviewing and editing this manuscript.
Once a couple is diagnosed with infertility, clinicians suggest a plan of care that is the most effective, least invasive and, whenever possible, economical. On a parallel journey, the couple also explores interventions or actions, on their part, that can contribute to their success in achieving a pregnancy, often researching complimentary medical techniques such as acupuncture.
In the U.S. over the last few decades as subfertile patients search for complimentary and alternative adjuncts to Western medicine in order to improve reproductive outcomes.
Acupuncture is an important arm of traditional Chinese medicine that has been used for centuries to regulate the female reproductive system. It has gained popularity In the U.S. over the last few decades as subfertile patients search for complimentary and alternative adjuncts to Western medicine in order to improve reproductive outcomes. Early studies regarding the effect of acupuncture on In Vitro Fertilization (IVF) pregnancy rates were promising, generating a large interest in this therapy among couples experiencing infertility. Since then, studies were undertaken to lend credence to earlier reports that acupuncture can have a positive impact on reproductive outcomes for fertility patients. Recent studies and meta-analyses, though, show mixed results, tempering our haste to encourage subfertile couples to devote their time and resources to acupuncture if its effects on fertility are not proven.
Mechanism of Action
Acupuncture is based on the principle that the body thrives when Qi (a form of energy) is allowed to flow freely through it. Conversely, when Qi is blocked or stagnant, it can lead to illness and/or malfunction. Along the body are energy points, called acupoints, which are situated along meridians (channels of energy) and are linked to certain body systems. By inserting, manipulating, and retaining very fine, sterile needles in the body one can stimulate these acupoints potentially correcting an imbalance of Qi, either an abundance or a deficiency. Manipulation of the needles can be done manually or by using low current or frequency to stimulate them.
In reproductive health, a few plausible mechanisms of action of acupuncture have been identified. One is that it works by inhibiting central sympathetic nervous activity which can cause an increased blood flow to the ovaries and uterus, potentially improving oocyte quality and uterine receptivity respectively. Acupuncture induces neurotransmitter secretion, activating the release of gonadotropin-releasing hormone, which can regulate the menstrual cycle, influencing reproductive hormones and potentially restoring ovulation in anovulatory patients. Finally, through its effects on increasing endogenous opioid production, it can reduce anxiety which, unequivocally, is experienced by infertility patients and may even negatively impact their reproductive performance.
Research on Acupuncture and Reproductive Outcomes
Although researchers have attempted to study the effect of acupuncture on reproductive outcomes, the results are inconsistent and the study designs fraught with methodological issues. There doesn’t seem to be continuity among the existing studies in terms of the timing and number of treatments, the proper control group and outcome measures. Early studies on the effect of acupuncture and pregnancy rates after an IVF cycle seemed promising and focused on the patient receiving two sessions, immediately before and after transfer. These were pilot studies, with small sample sizes, and the control and experimental groups were not similar enough in their characteristics (age, reproductive history…etc) to prove that it was solely acupuncture that had a positive effect. As stated above, one of the limitations of acupuncture research is defining the control group. Some argue that the control group should consist of women who have no intervention, whereas others believe it should be women who have ‘sham’ acupuncture, where they perceive that they are receiving treatment, they have needles placed, but they are not placed deeply nor on the proper meridian to be effective. Some studiesdo not show a benefit to acupuncture over sham acupuncture, and practitioners believe that it is because sham acupuncture is not inert. Several studies on pain comparing acupuncture with sham show that sham acupuncture still evokes a physiological response, strengthening the argument that it is an inadequate control and contributes to confusion in the literature. In addition, during their treatments, patients are still getting acupressure (when applying the needles) and also benefiting from a positive provider-patient interaction in a quiet room which can decrease stress, increase relaxation and possibly improve outcomes. As a result, most practitioners feel that comparing acupuncture to usual care may be a more useful control.
Presumably, researchers should replicate how a certain treatment or therapy is executed in clinical practice as much as possible in order to assess its applicability, but there is a disparity between the way that acupuncture is performed on participants in clinical trials versus how practitioners actually perform acupuncture in a clinical setting. For example, in clinical trials, the acupuncture points are fixed in order to adhere to rigorous study design. In real-life, though, practitioners prefer to personalize their protocol according to the patient’s history and current needs. Like any therapy, acupuncture arguably works best with regular sessions with a trusted practitioner. The early studies used a much lower dose of acupuncture, only two sessions: one immediately before and one immediately after the embryo transfer during an IVF cycle, now termed the ‘Paulus protocol’ after the one of the researchers who performed the study. Although initial results were promising, follow-up studies suggest that only two sessions isn’t sufficient to alter reproductive outcomes (though the effect on reducing stress can be immediate). In fact, a meta-analysis that grouped and analyzed randomized, controlled trials on acupuncture performed within a day of embryo transfer found no benefit in those patients who use acupuncture vs sham or usual care. Multiple treatments prior to, on the day of, and after transfer might increase pregnancy and live-birth rates, but future trials are necessary to determine the minimal number of sessions, as the dose of acupuncture needed will depend on the particular patient and her diagnosis.
…if someone’s first experience with acupuncture is in the midst of an IVF cycle (when she is already submitting herself to a series of injections)the thought of unnecessary needles (no matter how small) may make the idea of acupuncture less savory.
The optimal timing of the sessions is also not well-defined. Arguably, if someone’s first experience with acupuncture is in the midst of an IVF cycle (when she is already submitting herself to a series of injections) the thought of unnecessary needles (no matter how small) may make the idea of acupuncture less savory. Also, having acupuncture performed by someone with whom she is unfamiliar might actually be stressful for the patient, increasing anxiety as opposed to relieving it. In fact, one study showed lower pregnancy rates in the acupuncture vs control group when acupuncture was solely performed on the day of transfer and at an offsite location. In contrast, an observational study using the same acupoints as the previous study, did not find lower birth rates and, in fact, found higher live births in donor cycles. As a result, when possible, patients should consider starting acupuncture prior to their treatment cycle, have treatments close by or in the infertility center, and have regular sessions throughout with the same practitioner.
There is also disagreement regarding how to define ‘reproductive outcome’. For example, there is some data to suggest that acupuncture, and specifically electroacupuncture, might be helpful in cases of endometrial insufficiency by reducing uterine artery blood flow impedance and for pain relief. Some patients even choose to use electroacupuncture for pain reliefduring oocyte retrieval instead of anesthesia. Many of the earlier studies looked at more traditional metrics for reproductive outcome, such as clinical pregnancy or ovulatory rates but, ultimately the goal of fertility patients is to have a baby. Very few studies report live births and a recent prospective one showed that acupuncture was not better than clomiphene, in this regard, for PCOS patients.
Acupuncture and Stress Reduction for Fertility Patients
…some methods of stress reduction, such as having a glass of wine or exercising vigorously, are off limits during a treatment cycle and in the preconception period. Acupuncture, in this context, can be a powerful weapon…
Most would agree that infertility patients are both stressed and vulnerable and have greater levels of anxiety and depression than their age-matched counterparts. There is some concern that stress can contribute to infertility, so reducing stress in this patient population is critical. Also, some methods of stress reduction, such as having a glass of wine or exercising vigorously, are off limits during a treatment cycle and in the preconception period. Acupuncture, in this context, can be a powerful weapon as studies have found that acupuncture can help reduce anxiety. Even when researchers have not found a difference between control groups and those receiving acupuncture on pregnancy outcomes, many of them have still found that the acupuncture group has a reduction in anxiety levels, as evidenced by decreased serum cortisol levels or decreased perceived anxiety. It is recommended that stress reduction occurs, whenever possible, prior to the start of an IVF cycle, and that reducing stress might reduce the number of treatment cycles needed for pregnancy to occur. Although many infertility centers now offer more mainstream options such as in-house counseling or support, some have found that only few patients make use of this resource. Clinicians can capitalize on patients’ interest in complimentary medicine and suggest acupuncture in the context of providing emotional support, rather than limiting the definition of the desired outcome to be solely achieving a pregnancy. Acupuncture can help patients develop resiliency and cope with the day to day stressors and potential negative outcomes which often accompany treatment cycles. Stress and anxiety are often the cause of discontinuing infertility treatment, so even in the absence of unequivocal results in terms of hormone balance or increasing implantation rates, the ability to manage these emotions would still be incredibly beneficial to fertility patients.
Acupuncture in Pregnancy
Many patients are concerned about the safety of acupuncture in pregnancy. Acupuncture is often regarded as safe in the general population when performed by a licensed provider. Studies on the effects of acupuncture during pregnancy are few, but a recent literature review found that acupuncture during pregnancy was associated with very few adverse effects, and that all evaluated were unlikely to be caused by the acupuncture treatment. Some acupressure points can stimulate uterine contractions, so it is obviously important that these are avoided before and during pregnancy, but acupuncture can be very effective for relief of some pregnancy symptoms, such as lower back pain, headache and nausea, so it would be reasonable to continue treatments once pregnant. As there is much variability among providers, it is recommended that acupuncture be performed by a therapist with experience in reproductive endocrinology and health. When searching for someone, one recommendation would be to ask the staff at an infertility center or OB/GYN office whom they recommend. Another is to search for a practitioner who is registered with the American Board of Oriental Reproductive Medicine (ABORM.org) where he/she has to pass rigorous testing in order to be certified or The National Certification Commission for Acupuncture and Oriental Medicine (NCAAOM.org).
Despite increasing use of acupuncture by fertility patients, its ability to improve pregnancy or live birth rates has not been proven in the literature. Although its mechanisms of action on the female reproductive system seem plausible, the clinical trials studying it are so flawed that accurate interpretation of results is limited. The question arises, then, if we as healthcare professionals should be recommending acupuncture to our patients who might be short on finances or the time needed for regular sessions, particularly if its ability to enhance reproductive outcomes cannot be determined.
For infertility patients, acupuncture can provide balance and control during a journey short on both.
Arguably, though, maybe it’s time to redefine ‘reproductive outcome’ and instead of focusing on just clinical pregnancy rates as the ultimate measure of success, one should equally weigh the sense of control and reduced anxiety that is experienced by patients who undergo acupuncture. For infertility patients, acupuncture can provide balance and control during a journey short on both. One can argue that Eastern medicine has existed successfully for thousands of years, even if it is not amenable to the application of rigorous study design or statistical analysis. For this body of research, it might be reasonable to suspend the need to measure and demystify acupuncture and its effects and allow ourselves to appreciate its possible impact without measuring it.
Ovarian Reserve Testing and Diagnosing Diminished Ovarian Reserve
Dayna Browning, BSN, Jennifer Dwyer, BSN and Monica Moore, MSN, RNC
Edited by Paul Bergh, MD
A woman’s ovarian reserve refers to both the quantity and quality of her eggs, and diminished ovarian reserve means either or both of these factors are declining.
Ovarian reserve testing specific for the quantity of available oocytes consists of biochemical and ultrasonographic tests that represent a snapshot of where a woman falls along this continuum.
Surprisingly, women have the most eggs (oocytes) when they can least use them, prior to birth as a 20 week fetus! After birth, this oocyte pool dwindles until very few remain at the time of menopause. Ovarian reserve testing specific for the quantity of available oocytes consists of biochemical and ultrasonographic tests that represent a snapshot of where a woman falls along this continuum. It’s critical to have an accurate assessment of reproductive potential when planning for pregnancy, whether utilizing advanced reproductive technologies (ART) or not. When proceeding with ART, ovarian reserve testing dictates stimulation protocols to avoid unwanted outcomes, like cycle cancellation or ovarian hyperstimulation. Nurses are often the ones who interpret and review these results with patients, so in this article, we will explore the available tests, their applicability and pitfalls, and how best to discuss with the outcome with patients.
Egg Supply Diminishes with Age
Regarding the quality of oocytes, the millions of eggs that represent a woman’s oocyte pool are dormant for years, arrested in meiosis (cell division for sex cells). The next time these oocytes are re-activated and meiosis resumes is after selection within the dominant follicle, at the time of ovulation with the luteinizing hormone (LH) surge. So, at the time the oocytes are expected to resume cell division, they may have been paused in the middle of cell division from 13 years to as many as 40+ years. Cell division is a process that requires a significant amount of energy. As eggs age, so do does the cell machinery that is crucial for efficient cell division. Accordingly, aging oocytes may not respond as well as younger eggs once recruited from the original supply. These older oocytes are less effective at correctly completing meiotic cell division and thus are at an increased risk for aneuploidy (an abnormal number of chromosomes in the embryo, which is often lethal).This is often the cause for the exponential decline in fertility and increase in miscarriage rates seen in women who attempt to conceive in their later reproductive years. This decline in the oocyte’s ability to complete meiosis error-free is a reflection of oocyte “quality” and, other than a women’s age, there is no way to evaluate the chance of oocyte meiotic error.
Regarding quantity, the rate of follicular depletion varies considerably among women. Chronological age is an important factor when counseling infertility patients, but it’s important to note that two age-matched women can have very different levels of ovarian reserve. Although some lifestyle choices, such as smoking, trauma from surgery, or radiation/chemotherapy can be detrimental to oocytes, exercise and a healthy diet are important, but not necessarily protective. The fact that a fit, active woman in her 40’s can still have diminished ovarian reserve demonstrates the inescapable reality of ovarian aging.
The fact that a fit, active woman in her 40’s can still have diminished ovarian reserve demonstrates the inescapable reality of ovarian aging.
Diminished ovarian reserve (DOR) is a term used to denote that the decrease in the oocyte pool has reached a level in which it impairs fertility. DOR occurs even in women with regular menstrual cycles. Those who are diagnosed with DOR can be counseled that they will have a lower response to stimulating medications, a higher cancellation rate, and a lower chance of pregnancy after an IVF cycle than an age-matched woman whose ovarian reserve testing is normal.
Although it would be helpful if ovarian reserve testing reflected both the quality and quantity of the oocytes that remain (and are available for that particular patient), there is a stronger association between the outcome of the tests and the quantity of oocytes available, not their quality or competence. Research on the predictive value of the existing tests is mostly undertaken in the setting of a high-risk population, i.e. those who present to infertility centers, and caution should be taken when extrapolating these results to a low-risk group, such as women who have not been diagnosed as subfertile. The applicability of the results, then, should mostly guide clinicians about expected outcomes during ART cycles, for example, response to stimulating medications, possible cycle cancellation, and the chance for pregnancy after a treatment cycle. They are less reliable when used to predict the probability of a natural pregnancy or when menopause will occur. Also, no single test is predictive of reproductive potential and the patient’s medical history and clinical picture should always be considered when interpreting results.
Historically, a follicle stimulating hormone (FSH) level on cycle day 2-4 was used as the ‘gold standard’ of ovarian reserve testing. FSH is produced by the pituitary gland and is an important hormone necessary for follicle growth, particularly small follicles. As a follicle grows, it produces estradiol (E2) and inhibin B, and the increase in these hormones decreases the release of FSH from the pituitary. So adequate early follicular levels of E2 and inhibin B maintain FSH at normal levels. E2 and FSH levels are inversely proportional, so lower E2 levels would signal the pituitary to increase the production of FSH. As a result, it is important to also draw an E2 level when an FSH is drawn to assure that E2 is not elevated (>60-80 pg/ml) which would falsely lower FSH. As women age, the quantity and quality of the follicles that they produce declines. A poor-quality follicle (or a reduction in the number of follicles) results in an E2/inhibin B levels not high enough to provide negative feedback to the pituitary to reduce the production of FSH, so it is over-secreted. Consequently, elevated FSH levels on day 2-4 can be an indicator of diminished ovarian reserve. An FSH level >10 mIU/ml, according to the World Health Organization (WHO) 2nd international standards, is considered a sign of decreased ovarian reserve. FSH alone, though, seems to be a limited measure of ovarian response. It’s specificity and sensitivity vary in the literature, and it’s a poor predictor for pregnancy and live birth, particularly for young (<35 y/o) patients. As a result, most clinicians do not rely on this level alone when counseling patients.
A dynamic measure of ovarian reserve, that has been used in the past but is no longer widely used, is a clomiphene citrate challenge test (CCCT). Women undergoing this test have an E2 and FSH level drawn on day 2-4 of their menstrual cycle. Then, 100 mg of clomiphene citrate is taken orally on days 5-9, and an FSH level drawn on day 10. This has been termed a ‘stress test’ for the ovaries as it might show how ovaries respond to stimulation and reveal more subtle DOR that may be concealed by using a static test/single level. This test is in effect a bioassay of the inhibin B response of the follicle. Clomiphene citrate blocks estrogen’s negative feedback to the pituitary and the hypothalamus, however inhibin B produced by the follicles is not blocked by clomiphene citrate and is still recognized by the brain. In a normal CCCT test, with a sufficient inhibin B response, the FSH with the day 10 blood work should still be suppressed to the normal levels expected on day 3. Recently, though, other methods are increasingly used over this test as some feel that there is only a minimal to moderate benefit over testing FSH levels alone (if any) and is not necessarily cost-effective. As a result, some centers opt to use this test for patients in whom they suspect a poor response to stimulation (over the age of 35, I.e.) whereas others do not use this test at all.
Anti-Mullerian Hormone (AMH) is starting to emerge as the preferred measure of the quantity component of ovarian reserve. AMH is a hormone secreted by the granulosa cells that surround the early, small (up to 4 mm) follicles in the ovary. Normal levels are lab-specific, but many use >1.0 ng/ml as the cut-off. AMH expression is not gonadotropic-dependent, so can be drawn at any time during the menstrual cycle. Levels peak at 25 years of age and decrease with age (the opposite of FSH), with a level <1.0 mg/ml indicating diminished ovarian reserve and very low levels can be seen about 5 years prior to menopause. Elevated AMH levels also have clinical utility, as they would suggest a robust ovarian response, and have been shown to correlate with an increased risk of ovarian hyperstimulation syndrome (OHSS). AMH can be helpful in predicting the response to gonadotropin stimulation, and possibly pregnancy rates. The data is mixed regarding the predictive value of AMH levels and live birth, although there is some evidence that it might be better than FSH levels in this regard. Also, in women without a history of infertility, a prospective, randomized study found that low AMH levels do not predict a decrease in fecundity as compared to those with normal levels. AMH might also be useful in assessing the need for fertility preservation strategies. The data on AMH as being a reliable predictor of natural fertility is mixed, though, larger studies are needed to elucidate this.
As stated above, the follicles which become dominant and ovulate are just the ‘tip of the iceberg’ and demonstrate the immense attrition rate seen with normal human aging. Only 0.1% of oocytes present at birth make it to ovulation. Every month, a small portion of follicles (containing oocytes) are drawn from a woman’s egg supply in the hopes of being selected to become a dominant follicle. Around day 5-7 of a 28 day cycle, the follicle which has the most FSH receptors becomes dominant and the remaining follicles get reabsorbed by the body. Measuring the number of small (2-10 mm), antral follicles that are present by ultrasound on day 2-4, then, before dominant follicle formation, termed the Antral Follicle Count (AFC) is a helpful measure of ovarian reserve as it can be appreciated that the lower the overall egg supply, the lower the number of follicles available to be recruited. These are the follicles that contribute to the AMH level so it is no surprise that the AFC is highly correlated with AMH levels. This is supported in the literature as women with a lower AFC are more likely to have cancellation for poor response in IVF cycles. The literature is mixed regarding with the lower limits for AFC are, there is some agreement that less than a BAFC of <3-6 is concerning.
Poor AFC
Poor AFC
Normal/Good AFC
Good AFC
Although not well-established until the last decade, AMH and AFC seem to be emerging as the best approaches to procreative testing, as they are the most accurate in predicting poor response to IVF (better than FSH). They are also better at predicting hyper-response and elevated levels of either should alert the clinician to the possibility of OHSS. Although AMH seems to be superior to FSH in predicting live birth, data is conflicting regarding its ability to predict miscarriage rates.
Treatment of DOR
Very few treatment options are available when a woman has been diagnosed with diminished ovarian reserve. One reasonable, and affordable, strategy is advising the patient to begin supplements such as DHEA (Dehydroepiandrosterone) and Coenzyme Q10. DHEA is in a class of steroid hormones known as androgens which are at peak levels in humans in their mid-20s. Coenzyme Q10 (CoQ10) is an antioxidant that your body produces naturally to use for growth and maintenance and plays a key role in mitochondrial function. There has been recent data that suggests DHEA improves ovarian function, increases pregnancy chances and, by reducing aneuploidy, lowers miscarriage rates. Similarly there is also data that Coenzyme Q10 can not only help preserve the ovarian follicle pool, but also facilitates ovulation of gametes able to support normal development. Other suggestions include maintaining a healthy lifestyle and avoiding factors that can impair fertility such as an elevated BMI and smoking.
Historically, it was thought that superovulating patients with diminished ovarian reserve gave them the best chance of pregnancy during a treatment cycle, but a growing body of research suggests that ‘mini’ or ‘mild IVF’ might offer outcomes similar to conventional IVF cycles. Conventional IVF consists of the administration of high-dose external hormonal injections with the goal of developing a large quantity of oocytes. These oocytes are retrieved during a surgical procedure and later fertilized with sperm in a controlled laboratory setting. In mild ovarian stimulation, or mini IVF, an oral ovulation induction agent such as clomiphene citrate or letrozole is initially used, followed by the administration of low-dose injections to stimulate follicular growth. Because this approach leads to less oocytes retrieved, it can be done with local anesthesia as opposed to general anesthesia. The cost is also less because less injections are used. When comparing conventional IVF and mini IVF, a study found that there is fair to good evidence that clinical pregnancy rates are not substantially different between two types of stimulation in women predicted to be poor responders.
Counseling the Patient
When couples begin their fertility journey they are seeking answers as to why they are unable to conceive or have been experiencing recurrent pregnancy losses. A comprehensive diagnostic workup is the first step to treatment and, for many women, it is found that they have diminished ovarian reserve. Receiving and accepting this message, and its ramifications, is incredibly difficult for patients. As REI nurses it is our responsibility to assist in counseling the patient on appropriate care measures based on their results. Although it is more common to see a decline in ovarian reserve in women over the age of 35, this unfortunately can affect women of all reproductive ages. If a woman’s ovarian reserve testing (hormone levels, follicle count) falls within a normal range, a less invasive option such as IUI (Intrauterine Insemination) may be recommended as first line treatment. However, if a woman is shown to have signs of diminished ovarian reserve (low AMH, high FSH, low AFC) she would need to be counseled on the importance of aggressive fertility treatment such as IVF to optimize her chance of success for a current and potential future pregnancy, the higher chance of cycle cancellation, and the lower chance of pregnancy when compared to women her age with normal ovarian reserve. It is important to share with the patient that as she gets older her reserve and egg quality/quantity will continue to decline. This is especially pertinent for women who want to have multiple children, so ovarian reserve testing results should be taken into context with the couple’s family-planning goals, such as how many children would they ideally like to have.
One of the most difficult and emotionally-charged treatment options to discuss with a patient is the potential need for OD or ED (Oocyte or Embryo donation), as it requires that she accepts the inability to use her own eggs and agree to use someone else’s, a huge shift in her family-building perspective and the loss of a life-long dream.
One of the most difficult and emotionally-charged treatment options to discuss with a patient is the potential need for OD or ED (Oocyte or Embryo donation), as it requires that she accepts the inability to use her own eggs and agree to use someone else’s, a huge shift in her family-building perspective and the loss of a life-long dream. When delivering this sensitive news to the patient or couple it is important to be forthcoming , but empathetic and sensitive as well (Review How to Deliver Bad News here). Realize that the patient needs to essentially grieve the loss of her fertility. When making this phone call, make sure there is adequate time to discuss results and answer any follow-up questions the she (or her partner) may have. So be prepared that this call might take more time and allow for that when planning your day. Setting realistic expectations for the patient in terms of recommendations for treatment and the potential for success is crucial. Keep in the mind that the patient may not readily accept your news and may have an understandably defensive or aggressive reaction. Reminding the patient that you are available as a form of support will allow them to express their feelings and concerns once they are ready. Offering additional support resources for the patient such as speaking with a social worker, or scheduling a follow up appointment with their physician can be offered as well.
Ovarian reserve testing provides important information regarding likely reproductive outcomes in infertility populations. AMH and AFC are emerging as the more widely used tests to evaluate the quantity of oocytes remaining. Evaluating the quality of the remaining oocyte pool remains elusive though is often correlated with age. Currently there is no real treatment for women with DOR, but supplements and personalized stimulation protocols are options. When ovarian reserve testing results are abnormal, nurses need to realize that this news can be devastating to a patient. As a result, time and care should be taken when making the phone call to deliver these results, considering the patient’s clinical situation and desire for family-building.
In about half of couples experiencing infertility, there is a male factor which either contributes to, or is responsible for, their subfertility. This common condition presents a challenge to Reproductive Endocrinology and Infertility (REI) nurses as it is a complicated diagnosis with many causes and treatments and our formal education on the topic is, arguably, limited. This lack of information (combined with the reduced visibility and familiarity of the male partner in the infertility setting) can result in nurse discomfort when discussing results and treatment options. Since the semen analysis remains the primary test for male fertility, and nurses are often the ones who are interpreting and discussing these results with patients. The goal of this article is to review the sperm cell itself, it’s journey through male and female reproductive tracts and how to interpret the semen analysis properly. The psychosocial aspects of male infertility will also be reviewed in an effort to improve nurse/patient communication when relaying results.
The Sperm and Sperm Journey
The sperm cell has one main role: to transfer paternal DNA by reaching, attaching to, penetrating and activating the female oocyte and its shape is highly adaptive to its function.
The sperm cell has one main role: to transfer paternal DNA by reaching, attaching to, penetrating and activating the female oocyte and its shape is highly adaptive to its function. A sperm cells consist of four main segments: The head (which contains the nucleus and the acrosome, an organelle which is critical for penetrating the zona pellucida of the oocyte); the neck (which contains centrioles); the midpiece (which contains the mitochondria, the energy provider); and the tail (which has flagellum that propels the sperm). Sperm cells are unique in that they mostly lack cytoplasm, which is extruded as they differentiate from round spermatids to mature spermatozoa with the typical shape with which we are familiar: a small oval head (mostly consisting of the nucleus) and a long tail. So, basically, a sperm cell is a small, energetic torpedo that delivers male genetic material. Sperm cells are produced approximately every 46-72 days by a complex process called spermatogenesis which occurs in the seminiferous tubules of the testes. Spermatogenesis is affected by intrinsic factors, such as a properly functioning hypothalamic-pituitary-testicular axis, and extrinsic factors, such as heat. In fact, the testes reside outside of the body in order to provide thermoregulation (they are 2-3 degrees cooler than rectal temperature). Once spermatogenesis is complete, the sperm enter the epididymis, a comma-like structure on the outside of the testicle, where they finish the maturation process and become motile. They remain in the epididymis for 2-3 months or until the time of ejaculation, which is an important point as sperm that is ejaculated was produced at least 2-3 months prior.
Image credit: Wikipedia.com
In order to travel through the female reproductive tract, sperm needs to combine with fluid in which it can move. This fluid is generated in the male by several structures: the seminal vesicles, the prostate gland and urethral glands and, once combined, called seminal fluid or semen. Semen also provides fructose, the energy source necessary for sperm movement, and other substances that protect sperm during its journey through the reproductive tract, as sperm cells are vulnerable to a myriad of external insults, such as temperature changes, acidic pH and oxidative stress.
The sperm journey through the female reproductive tract closely resembles an obstacle course, fraught with barriers and challenges, and a healthy sperm must be equipped to overcome them.
The sperm journey through the female reproductive tract closely resembles an obstacle course, fraught with barriers and challenges, and a healthy sperm must be equipped to overcome them. Once ejaculated, the seminal fluid provides substances that protect the sperm and assist it during its journey, such as agents which buffer the acidic environment of the vagina, substances that assist with motility through cervical mucus and still others which suppress the immune response of the female which can destroy sperm. Those sperm which survive to enter the fallopian tubes remain there for a period of time where the glycoprotein coating is removed from the surface of the sperm (called capacitation), a necessary process where sperm acquire the ability to fertilize an egg. The acrosome, the organelle covering the head of the sperm, is filled with the enzymes necessary to penetrate the zone pellucida of the oocyte, allowing one sperm to enter and fertilize and activate the egg. The remaining sperm die off in a process called apoptosis. There is a huge attrition rate from the sperm present in the ejaculate to those that reach the zone pellucida, so in order to account for this, many millions of motile sperm need to be deposited in the vagina at the time of intercourse in order for just tens of hundreds to reach the ampulla of the fallopian tubes, where fertilization usually occurs.
Diagnosis of Male Infertility
A comprehensive evaluation of the male has three necessary components: A thorough medical history (including a sexual and reproductive history), a physical exam, and a semen analysis, the main diagnostic test for male factor infertility. There seems to be agreement among most experts that the initial evaluation should include a medical history and a semen analysis and, if abnormal, then the patient should be referred to a male reproductive specialist with the expertise and experience to complete the physical exam.
The semen analysis is a snapshot of a male’s semen parameters at that moment in time. Its components include a microscopic assessment of sperm concentration, motility, morphology and the presence of round cells, debris or bacteria. Most REI centers follow World Health Organization (WHO) criteria from 2010 which provides the lower reference limits for each parameter. It’s important to note that a normal semen analysis doesn’t imply fertility and an abnormal semen analysis doesn’t imply subfertility. Historically, the percentage of motile sperm has been reported to correlate best with pregnancy outcomes, but it is now suggested that in order to properly interpret the semen analysis, one must use a combination of parameters as opposed to noting that one or two are low and diagnosing the male with infertility. Although some clinicians prefer two separate specimens obtained 1-3 weeks apart, the more recent consensus seems to be that one specimen is adequate unless the results are abnormal, then another specimen should be obtained with an emphasis on production specifics, such as assuring an ideal abstinence period of 2-5 days, and determining if there was any impediments to producing the sample, such as the male “missing the cup” during the collection process. The subsequent specimen is collected to account for the variability in samples seen within the same individual, not to determine if a treatment or therapy worked.
Most of the components of the semen analysis are self-explanatory, for example, motility describes the percent of sperm that are moving, although there are different levels of sperm progression from twitching in place to actively moving. Morphology refers to a subjective description of how the sperm appear (size and shape) under the microscope. There can be defects in any, and all, of three regions of the sperm cell: the head, neck or tail, which can affect the sperm’s movement or ability to penetrate the oocyte. Low levels of sperm concentration, motility or morphology theoretically imply that the sperm can be impeded in its ability to reach or penetrate the oocyte. Once inside the zona pellucida, though, the sperm should act normally to fertilize and activate the egg, hence the reason why ICSI can result in fertilization in the absence of any normal forms or very low motility.
ASRM Practice Committee: Evaluation of the infertile male, 2015
True to the definition of the word ‘component’ the different values of the semen analysis are just parts of the whole picture, each one not meant to be taken in isolation in order to appreciate an accurate clinical picture of the male patient. The motility and morphology are percentages and the total number of motile or normal sperm, respectively, should be taken into account before a diagnosis of male factor fertility is made. For example, 15 m/ml is the lower limit of concentration and 4% is the lower limit of morphology. If a semen analysis reveals 3% morphology, and the concentration is 15 m/ml that is more concerning than a semen analysis that shows a sample with 3% morphology, but a concentration of 100 m/ml.
There are some common terms utilized when discussing the interpretation of results. Oligospermia denotes a low sperm count (<15 million/ml) and severe oligospermia is when there is <5 million sperm/ml. Azoospermia is absence of sperm in the ejaculate. Azoospermia is further segregated into two categories: obstructive azoospermia (where sperm is being produced but not delivered, such as a male who had a vasectomy) and non-obstructive azoospermia where sperm is barely being produced if produced at all. In the case of severe oligospermia or non-obstructive azoospermia, it is recommended that a karyotype is obtained on the male to rule out genetic abnormalities. Some experts suggest obtaining a karyotype in cases of oligospermia where the sperm count is <10M/ml based on the fact that chromosomal abnormalities are more common in infertile men than in those who are fertile. Asthenospermia denotes poor sperm motility while teratospermia refers to poor sperm morphology.
Male infertility terms
Consequently, the semen analysis is an important test but it’s critical to note that it is capturing a biological process at a single moment in time. As a result, there are limitations to its diagnostic and prognostic value. For example, it may show that the amount or shape of sperm are adequate, but it doesn’t assess for the functionality or fertilization potential of those sperm. Also, solely relying on its results can cause one to miss significant conditions or behaviors that can contribute to infertility, such as sexual dysfunction.
Although not yet standards of care, some clinicians utilize additional tests that might uncover damage to sperm that is not revealed in a basic semen analysis, such as DNA fragmentation. DNA integrity is important for normal embryo development. Although more data is needed, a growing body of evidence suggests that high levels of DNA damage can negatively impact reproduction. Sperm samples from infertile men have been shown to have significantly more DNA damage than those from fertile men. Damage to DNA of sperm occurs during their development as well as during the maturation and transport process that takes place outside of the testes. DNA damage can also be due to external factors such as oxidative stress, heat and significant varicocele. The American Society of Reproductive Medicine (ASRM) position The clinical utility of sperm DNA testing states that although some couples may benefit from this testing, it is not recommended for routine use. It also warns that the predictive value for clinical treatment is undetermined and there is no agreed-upon treatment once DNA damage has been diagnosed.
Similarly to unexplained infertility in females, about 30% of men have unexplained or idiopathic infertility as clinicians are unable to determine an apparent cause using the investigative methods described above. Currently, oxidative stress (OS) is believed to be an important and plausible cause of idiopathic male infertility. Simply put, OS reflects an imbalance between reactive oxygen species, which are harmful to the body, and the body’s ability to defend itself (antioxidant defenses). Sperm are susceptible to oxidative stress because they lack the necessary cytoplasmic-enzyme repair systems. OS can result in poor fertilization, poor embryonic development and pregnancy loss. Some examples of OS include poor lifestyle choices such as smoking and excessive alcohol consumption. Others include infection, radiation and high-grade varicoceles. Prevention and management of OS includes diagnosing and treating infection; minimizing detrimental behavior (such as the lifestyle choices listed above), limiting exposure to heat, toxins and heavy metals and ensuring the consumption of anti-oxidants in one’s diet. Additional studies are needed to elucidate the effects of taking anti-oxidants as supplements. Some studies suggest that they may increase sperm parameters, while others find that the data or study design is limited.
Psychological Effects of Infertility on Men
Certainly, whenever communicating with patients, their perspective should be taken into account when delivering results and reviewing and discussing semen analysis results is no exception. Consider the following unique characteristics of men in an infertility setting. They often feel excluded or minimized during the fertility process, even their own lab results are usually reported to their female partner. In addition to the emotional stress that is intrinsic to fertility treatments, men also share the burden of the financial aspect of fertility treatments, which can be costly and can deteriorate the couple’s savings over time. Men in an infertility setting often feel like a failure. The inability to impregnate their partner can be emasculating, regardless of if the fertility factor is male, female or both, which can lead to a compromised sense of identity.
True to the nature of fertility, even the studies available that focus on the mental health of the male partner in an infertile couple are disproportionately low compared to those of the female partner, but the few that exist confirm that mental health in men is compromised as a result of infertility.
The fertility process itself, and repeated negative outcomes, can lead to depression and anxiety in men as well as women. True to the nature of fertility, even the studies available that focus on the mental health of the male partner in an infertile couple are disproportionately low compared to those of the female partner, but the few that exist confirm that mental health in men is compromised as a result of infertility. A recent one found that 15% of male partners who did not have a successful pregnancy during the study interval met the criteria for being depressed Another group of researchers studied 274 infertile men undergoing treatment and found that 32% were diagnosed with depression and that more than 60% met the clinical criteria for anxiety. Also consider that the couple’s relationship with each other can fall prey to the stress of infertility, particularly if a pregnancy is never achieved. According to one study couples for whom fertility treatments failed were three times more likely to divorce than those who had a child. In addition, the stress of infertility can lead to sexual health problems in the male, like erectile dysfunction, which can hinder treatments, and cause considerable relationship discord, particularly if he is unable to produce a sperm sample on command.
So, what can nurses do? Researchers recommend that health care providers actively involve male partners in the treatment process. Educating themselves on the male perspective is a valuable first step. A plan should be made in advance regarding how, when and to whom the couple would like male results to be delivered. Realize that men communicate differently and that the male partner may not be as familiar with the clinic’s systems and protocols, for example he may not know the password to access a patient portal in order to obtain his results and must rely on his female partner to do so. One study found that men prefer oral to written communication, but realize that similarly to the female, the male partner is most likely at his job, and can’t listen actively or speak freely. It would be preferable to set up a time in advance to call, maybe during his lunch hour or on his way home from work, if possible. Consider offering mental health support to male partners, but do not be surprised if it’s declined. This same study found that men prefer to have support from infertility clinicians as opposed to mental health professionals.
Male factor infertility is a prevalent issue among infertile couples. The diagnosis can be complex, but at the very least, should include a comprehensive medical history and semen analysis. The semen analysis, although a useful tool, should be interpreted carefully and comprehensively, and in consideration of the entire clinical picture. Other, more specific, tests for male fertility might be useful, but are not yet standard of care. Infertility is stressful, regardless of the cause. Often forgotten, or his presence reduced to only occasional or infrequent contact, the male should be involved in the fertility process whenever possible.
Earlier this month, we were honored to be speaking to Dr Helen Riess about the important concept of empathy for healthcare providers (See her TED talk here). Dr. Riess is Co-Founder and Chief Scientific Officer of Empathetics. She is an Associate Professor of Psychiatry at Harvard Medical School. Her research on empathy and the neuroscience of emotions has been published in peer reviewed journals, and she is a core member of the Research Consortium for Emotional Intelligence (CREIO) as well as a faculty member of the Harvard Macy Institute.
Monica Moore: Thank you for taking the time to speak with us today. Our field, of reproductive endocrinology and infertility (REI), is constantly evolving with exciting new advances that continue to improve pregnancy rates, but we are still not at 100%, so often as REI nurses, we find ourselves often having to give bad news to a patient population that is both incredibly savvy and stressed, without having been properly trained in delivering this news. I’m so happy to talk to you today about how to impart bad news sensitively and in a way that helps our patients.
Helen Riess, MD: Hello and happy to talk to you today.
MM: As discussed, the REI field is not life-threatening in the true sense of the word, but it is life-altering to our patients.
HR: I agree, for them it is life-altering as it could mean the end of a dream.
MM: Yes. In keeping with this, can you give us a brief overview of the role of empathy in patient interactions, particularly when delivering bad news? Can you give us an example of a few empathetic statements?
HR: The preparation for giving bad news really begins with the provider, who has to be mindful that she is the messenger of bad news. He or she needs to think: “I am not the bad news myself, but how I convey it is what this person will remember”. Really, it helps to put yourself in the patient’s shoes and think, “How would I want this news delivered to me?”. That is a starting point. I think that the role of empathy is both emotional and cognitive resonance. The emotional part is to consider how hard it is to hear this news or how disappointed they will be. The cognitive perspective includes considering what this news is going to mean for this patient’s life. In this sense, it is helpful to have some information about the patient. Is this the patient’s fourth or fifth attempt to conceive as opposed to the first time, when they know that they have a few more chances? What about the patient’s age? Is she 45 or 46 or is she 36? Is this the patient or couple’s last attempt, so that this news maybe the end of the wish and the hope to have children at all. The cognitive perspective is really important to consider not just what this experience would be like for you, but what would it be like for this patient. Both the emotional and cognitive component are crucial.
The important concept about delivering bad news is that people are going to remember more about how you said it than what you said.
You would want to avoid bluntness and deliver the news in a way that doesn’t feel uncaring or perfunctory. Realize that even though you might say “Sorry, you are not pregnant” ten times a day, this is the first time this person is receiving the bad news. We recommend using an empathic bridge statement, such as using phrases like, “I wish I had better news to share” or “Unfortunately, the test results came back in a way that I think is going to be very disappointing to you”. I think we all have witnessed bad news delivered bluntly. The important concept about delivering bad news is that people are going to remember more about how you said it than what you said. Everyone who is struggling with infertility already knows that there is a possibility that it won’t work, so it won’t be a shock, but what they really need is someone who is offering care and compassion. We say that infertility is not a terminal diagnosis, but in a way, it is. This is the end of many people’s hopes and dreams. Bad news is really any news that permanently affects your vision of how you were going to live.
Bad news is really any news that permanently affects your vision of how you were going to live.
MM: One of our dilemmas as REI nurses is that we have certain information that we need to convey during the phone call, such as, “Please call us with day 1 of your next period” or “Schedule a consult with your physician once you are ready” and sometimes due to our discomfort or need to impart that information, we rush the delivery. Also, often, we have to relay bad news over the phone (negative pregnancy tests or pregnancy levels not increasing appropriately, for example). We are obviously unable to use non-verbal strategies to empathize, but what can we say or do in these situations that would be helpful?
HR: It is much more difficult when you can’t see if a person’s eyes are misting or what their facial expression is so that you can respond in an appropriate way. One of the ways to manage this is to acknowledge this. Saying something like, “It’s really unfortunate that I have to deliver this news over the phone because I can’t see your response, and I know that this is a lot to take in, but we can pause right now to let this sink in and I’m here at the other end of the line while you process this”. So, invite the pause. Many people rush to fill in a void because they are nervous or afraid to hear that the person is upset, but if you can frame it using the statement above, I think that the more that we convey our limitations; the more we are overcoming them.
MM: I’ve never thought of saying that, because it feels like stating the obvious, but that makes a lot of sense.
HR: It is obvious, but it is allowing the awkwardness to be awkward. If you have psychological support available at your clinic, you can also say, “We have support staff right here at our clinic that are available to help you deal with the emotional disappointment of this”. You don’t have to use the word psychologist or social worker, but really refer to them more to what their function is, which is to support the patient. Also, you don’t want to use the words “depression” or “cope” which might make the patient feel that they are having an abnormal reaction or response.
MM: I find that a 2 second pause feels like a 20 second pause. I tried it the other day and, it felt awkward and was difficult to not fill in the space with unnecessary chatter.
HR: I think it’s important to frame what you are doing, such as saying “I know this is difficult to do over the phone, but I want to take a moment to pause to let this sink in” so that the patient knows that you haven’t just gone silent over the phone.
MM: Just to add some more complexity to this situation, in some instances, the person who is delivering the bad news does not know the patient well, for instance, the patient’s primary nurse is away that week or their physician is in surgery and another, covering physician or nurse makes the phone call. Obviously this is not ideal, but any suggestions for how to proceed with this difficult conversation when a strong relationship doesn’t exist between patient and provider?
HR: I think stating the situation, which is “Hi, my name is Monica Moore. I’m calling from xyz clinic or Dr X’s office. I know that you don’t know me, and I wish that your doctor or nurse was available to be making this call, but we discussed it and we thought it might be better to give you the information, even though you don’t know me well, so that you are not anxiously awaiting the news”. Maybe it makes sense to give the patient a choice, preferable in advance, such as “Would you rather hear the results as soon as possible or would you rather wait and hear them from someone from your team who knows you better?” Be transparent about the situation because it gives the patient a choice.
…the more that we convey our limitations, the more we are overcoming them.
MM: Sounds like it’s best to be proactive in this situation. If a nurse knows that she has a patient who is going through a difficult time, has had many losses or failures, or is emotionally labile (we probably can all identify our patients like this easily) to have this conversation in advance. For example, one of your patients will be having her pregnancy test on a Thursday, and the nurse knows that she is off on Thursdays. What I’m hearing from you is that it would be best to talk to the patient prior to the pregnancy test and let her know that you are off that day and to mutually decide how she would like the news to be delivered.
HR: I think you are absolutely right. The more that you can share the dilemma with the patient and empower them to let you know what they want, then they have the choice. The nurse delivering the news can still say “I wish you could be hearing the news from someone who knows you better” as the empathetic bridge statement.
MM: what you told us so far has been incredibly helpful. I think we sort of know some of these strategies but to what extent we put them into practice on a regular basis, I question, even in my own personal experience. What resources are available for us to utilize so that we can learn and practice these strategies?
HR:Empathetics has a “delivering bad news” module. It is about an hour and it’s all about delivering all kinds of bad news. We review verbal and non-verbal aspects and how to manage your own anxiety. It’s accredited for nurses to get CEU’s (and also for physicians). It’s an interactive, online course, so people have to listen to different scenarios and make choices. Sometimes it’s helpful to see all different scenarios where someone maybe delivers the bad news in a way that’s not ideal. Some people can relate to seeing what not to do as a learning point. We have a whole suite of empathy training that talks about difficult patients, how to have empathy…etc. Those resources are there. We offer in-house specific training in empathy as well.
MM: As you are talking, I’m thinking that one strategy that we can use is role-playing. I’m sure that you use this in your practice. Maybe the newer/novice nurse acts as the ‘nurse’ and the experienced nurse is the ‘patient receiving the news’.
HR: Absolutely. We offer manuals that train facilitators to do this where the role-playing situations are basically spelled out. What kind of reactions can you expect and how do you draw these reactions out of people so that you can address them? We can send a trainer there or you can send your team to use and we can teach you how to offer these facilitator workshops. It’s exciting to see people understand that this is about managing the whole person, not just the biology of getting pregnant.
MM: We really appreciate your time and input, thank you so much for speaking with us today.
HR: Thank you for having me, my pleasure. If you would like more information about empathy training, please email dblake@empathetics.com.
Everyone would agree that functionality of the uterine lining is incredibly important for implantation of the blastocyst to take place. The question of how to measure this, termed ‘uterine receptivity’, has been studied extensively in the literature. The methods that have been used in the past were indirect, assumptive and not reproducible. Researchers in Spain have created a new tool which has been shown to be promising for identifying molecular markers for uterine receptivity.
Remarkably, as the blastocyst floats within the uterine cavity looking for a place to land, a dialog takes place between the blastocyst and the endometrium. In order for a successful implantation to take place, the blastocyst needs to be at the appropriate stage, and it needs to signal the uterine lining to ‘accept’ it. Within the uterine cavity, once ready for implantation, the microvilli present on the trophoblast cells of the blastocyst act as one side of ‘velcro’ to adhere it to the uterine lining. The embryo is in search of a receptive endometrium (the other half of the velcro) which will ‘fasten it’ to the uterine wall. The hormonal preparation of the uterus plays a critical role each month in creating this environment in which the blastocyst can adhere to the endometrium in the hope that implantation will take place.
The uterine lining undergoes changes during the two phases of the menstrual cycle that prepare it for blastocyst implantation. During the proliferative phase, it grows due to the increasing production of estrogen by the ovaries. The second phase is called the secretory phase where the production of progesterone, produced by the corpus luteum, converts the endometrial lining to a secretory one, changing the cells to prepare for implantation (a process called decidualization). Should implantation not take place, the hormone levels will fall, resulting in a shedding of the lining, which results in menses. Studying the mid-secretory phase is of great importance since the window of implantation (WOI) takes place then. The sweet spot of WOI is approximately a 2-day period when the uterus is prepared to accept the implantation of a blastocyst. Conventionally, it was assumed that every woman had the same WIO, (approximately 8-10 days after ovulation) so embryo transfers would be scheduled to take place during this time. This theory has recently been challenged, with researchers proposing that the WOI can vary among women.
Research has been done extensively to detect and determine criteria necessary in order to call an endometrium ‘receptive’. In the past, this was done using histological criteria, i.e. the microscope appearance of the endometrium (termed the Noyes Criteria). Certain days of the menstrual cycle have typical microscopic characteristics and a pathologist would determine if the sample looked like day 16 or 17..etc (dates were reported with ovulation normalized to day 14-so an endometrium that was day 17 by Noyes Criteria should be 2 days post ovulation). As one can imagine, there is much variability and subjectivity in this interpretation between pathologists, plus womens’ cycles can show considerable variability. Also, just because the cells have the appearance of a typical cycle day 16, for example, doesn’t mean that the lining is actually receptive. That would just be implied. As a result of these limitations, and some recent studies that found this morphological dating method to have poor predictive value, this method of assessing uterine receptivity is no longer widely used.
One can also look at the appearance of the lining by ultrasound in the late proliferative phase. Many studies have focused on the endometrial thickness and type (triple-line vs homogenous appearance). Although the lower limit of an acceptable lining has not been agreed-upon by researchers or practitioners (most would arguably be satisfied with a lining of 7 mm or above) that information is a reflection of the adequacy of the proliferative phase, which tells us that the lining was properly primed by estrogen, but doesn’t give us any information other than that. Ultrasound in the secretary phase is not helpful, as it shows a thick, homogenous lining that doesn’t usually affect clinical decision-making, so is not routinely performed.
Over the last decade, different ways of studying the endometrial lining more directly have been investigated, first by attempting to identify the substances that were generated at the time of implantation, the cytokines, adhesion molecules and other proteins. To date, this line of investigation has been unsuccessful, so the focus has shifted to the stage that leads to the production of these substances, the stage of RNA transcription. Transcriptomics allows the study of gene expression by looking at the mRNA produced. It can provide a molecular profile of the status of the endometrium by telling us what genes are actually “turned on”. Gene expression profiling is now widely used for other disciplines, such as tumor classification.
With the relatively recent advent of DNA microarray analysis we can measure the expression of thousands of genes simultaneously, allowing us to explore which ones are expressed in the mid-secretory phase, when implantation takes place. The discovery of this technology was a major turning-point in the study of endometrial receptivity and several studies were undertaken to determine which of these genes were important during the WOI. Researchers agree that there is a specific and unique action that takes place during the process of transcription, when RNA creates the ‘script’ for a protein, in order for the endometrium to become receptive, but the identification of the specific genes involved was elusive until recently. A group in Spain identified 238 genes related to endometrial receptivity and collected the data to create a tool, named the endometrial receptivity array or ERA (Diaz-Gimeno, et al 2011). This test purports to identify if an endometrium is receptive or not based on the mRNA profile or the endometrial gene expression. It further differentiates the non-receptive category into pre- or post-receptive) in natural or hormone-replacement (HRT) cycles, regardless of it’s appearance by ultrasound or under the microscope (histological). This group then applied their tool by testing it on patients with recurrent implantation failure (RIF) by performing a multi-center, prospective study. What they found is that the WOI was ‘displaced’ in 26% of the women with RIF, so in 1 out of 4 patients with RIF, dysynchrony between the blastocyst and the endometrium might be to blame (Ruiz-Alonso, et al, 2013). They then did a second ERA test on the patients who had the displaced WOI to confirm that by adjusting the progesterone start or transfer day (see more on this below) increased implantation rates. They performed a subsequent adjusted embryo transfer (termed a personal embryo transfer or pET) and demonstrated a 50% pregnancy rate and a 38% implantation rate in this group of patients (which is the rate similar to the control group who did not fail a treatment cycle). This data supports the concept that the conventional window of implantation differs among women (at least a fourth of us) maybe only slightly in some cases, but enough to preclude implantation.
The test is performed in the secretory phase of either a natural cycle or a hormone replacement (HRT) cycle. If during a natural cycle, then the biopsy is done on LH surge + 7 . If during an HRT cycle, then the biopsy is performed on exogenous progesterone start + 5 (120 hours post start of progesterone). The biopsy sample is sent to the lab and analyzed (this takes approximately 2 weeks) and results are termed either ‘receptive’ or ‘non-receptive’. If non-receptive, it further analyzes the sample as pre-receptive or post-receptive. If pre-receptive, then the patient needs more time (hours or days) of progesterone, so the progesterone is started earlier or the transfer is moved later. If post-receptive, then the WOI has already passed, so the recommendation would be to start the progesterone later or move the transfer earlier. The recommendation is to repeat the cycle after modifying it according to the suggested intervention (more or less days of P) and the biopsy is redone to confirm that the endometrial tissues sent now receptive. This step is center-specific with some practices often performing a repeat mock cycle with biopsy and others only occasionally repeating it, but still using the recommended progesterone modifications for the frozen embryo transfer cycle, thereby creating the patient’s personalized embryo transfer(called pET). For more information on the specifics of the results and testing criteria, see the video here.
Although the data collected so far is promising, there are some limitations in the study design that should be considered when interpreting results. One is that all of the studies performed so far have relatively small sample sizes. Another is that there was no effort (in most studies) to separate out the embryo quality so that this important variable could be controlled. (There is a recent, retrospective study, in Japan where the researchers only transferred back euploid embryos with optimistic results, but it was retrospective and had a small sample size.) Furthermore, in the initial ERA studies, the non-receptive group was not further stratified to include a segment who did not have pET prior to their next transfer, so it is not known if they would have been pregnant just due to trying again, without further intervention. Finally, keep in mind that if 25% of RIF patients had a displaced WOI, 75% did not, implying that there are other factors (embryo quality among them) that could be the cause of implantation failure.
The importance of determining the timing of endometrial receptivity has always been emphasized in reproductive endocrinology. Now, instead of just relying on the way the endometrium appears, either by ultrasound or microscopically, some researchers suggest that we have the added benefit of being able to study the molecular changes that happen within the endometrium and act on these results to form a personalized prescription for subsequent transfers. Although exciting, further studies are needed to confirm this small subset of studies and also to determine if this test will be useful for an expanded group of women (Currently it has been suggested that it should be offered to those who have failed >2 IVF cycles or >1 donor oocytes cycle.) Methods of non-invasive testing are also being explored and might be a viable option within the next decade. The idea that every woman has their own personalized window of implantation (and that we can determine and take advantage of this) is a new and exciting concept in REI.
Special thanks to Paul Bergh, MD, FACOG For his assistance with editing this article.
This photo was taken during the first hour of a seven-hour car ride that was as crazy and stressful as you can imagine it would be. My kids couldn’t seem to coordinate their bathroom breaks, there was bad traffic, and many, many squabbles in the car where I threatened some unmentionable actions and said things that I regret.
The calm before the sh*t storm
But you would never know just by looking at this picture. What would have been real and accurate is if I took a before and after photo, the ‘after’ taking place in the throes of crazy, when I was sweating and talking to myself. In fact, if I’m being honest, even though they start off well-intentioned, most of my long car trips end like this one, where we are all fighting and fussing. But we don’t show that stuff, those unvarnished emotions, to the world because they are deemed unacceptable. Instead, we process them, suppress them or package them up in a nice little box or, in this case, an acceptable picture. There’s a stigma, still, attached to being authentic and admitting that you are struggling.
In my role as an infertility nurse and nurse educator, I often function as a patient concierge, counseling people during their fertility journey. Some formally, but many people informally. I can’t tell you how many times I am approached by a friend who has read one of my blogs and asks me to talk to their daughter, family member or friend about what they should do when they are ready to conceive. I do talk to them, and I actually cherish these interactions, being able to demystify or explain complex processes.
Lately, I’ve been speaking to those who are not actively trying yet, and we discuss what they can do prior to pregnancy. I go over the basics, taking vitamins, getting immunized, achieving a healthy weight, but what I really want them to know is that preparing for pregnancy (whatever that path looks like for them) is an inside job.
Here is the irony about female fertility: You don’t know if you can conceive unless you try and you can’t try until you are ready to have a baby. There are no previews or glimpses into the important machinery that is the female reproductive system, so we can’t ‘prep’ for it until we are ready to ‘use’ it. This is a foreign and uncomfortable concept to most of us.
Think about our past experiences which form the context for this current one: we have an important test, we study for it. We are running a race, we train for it. You decide to start a family and you, well, go for it. Fertility (within reason and depending on age) follows a bell curve, like many processes in life, so that the majority of people get pregnant in a few months. Some get pregnant right away, and we know this because we are often inundated with these stories, like folklore. Most take a few months, and some need assistance from a fertility clinic to conceive. I can tell you, though, that I review lots of pregnancy records for my clients and a women might ‘remember’ that she got pregnant in a month, but the OB/GYN records state 3-4 months. It’s just all about perception.
Many of my friend’s daughters are reluctant to call me, either because they are embarrassed, or just don’t want to label that they are trying-because then, if it doesn’t work, they have failed at something. Many of them are ‘not not trying’, which I assume means not using birth control and having sex for fun instead of on certain days of the month.
Why do we, as women, feel ashamed or embarrassed to talk about this kind of stuff? Social media doesn’t help as it perpetuates a myth that everyone is happy, that situations are under our control most of the time and, when they aren’t, they are handled with humor and grace. If we are being authentic, we know this isn’t true and I am guilty of perpetuating this as well. I post pictures of my kids and my life (like the one above) that don’t truly reflect the fissures in it, posed pictures while everyone is smiling or funny ones where it seems like I’m laughing at something when I wanted to yell or cry. I still felt the frustration that the situation generated, but took the picture once it was over and processed. So, it probably never really got resolved, just repressed and reframed.
Why do we correlate importance with what’s visible?
This is what happens to young women who are struggling with infertility. They feel the anxiety of trying or wondering when to try, how to try, but then internally compartmentalize it so that they can seem ‘normal’ to their OB/GYN or family members. This is the snapshot that we see on social media, not the real person with real feelings. I talk about this with my patients.
One in particular is so incredibly put-together while she is on the phone, regardless of whether it’s good or bad news. But once, in an unguarded moment, she revealed to me that she is a ‘mess’ after she hangs up the phone. She’s not a mess. She’s a deeply feeling person in a messy situation. There is a difference. But I can reassure her many times and the message might be received but not heard, or heard but not absorbed.
I am working on a venture to develop strategies for nurses to help them find joy in their jobs. I am helping to write protocols, educate them and refine their systems so that they are more efficient. What I can’t emphasize enough, though, is that the women need to do the inner work.
External factors and stressors will always be present. We need to feel that we are good enough, strong enough, just ‘enough’ regardless of our path or outcome. I’m not an expert in this field, and am just beginning to study it. But I have spoken to a few who are well-versed in it, and here are some of the activities that they recommend for developing inner strength:
Journaling or writing. I started writing my blog posts as a form of stress release after a difficult patient conversation and find that they are just as helpful to me as they are to others. It was difficult for me to reveal how I felt on that car trip, and allow myself to be vulnerable, but vulnerability is a powerful tool, for more on this, read this excellent book by Brene Brown.
Going outside for a walk or exercise. It’s not just about the aerobic activity, it’s about the contact with nature and invoking your senses to try to get you to focus on the present moment. If the weather precludes outside activity, go to the gym to move, but smelling the leaves or feeling the sun on your face or putting your feet in the sand brings you back to the present. Nature can stop, if even only for a few moments, your mind from going down the well-worn path of would-haves and should- haves and endless ruminating and thought-looping in which we have a tendency to engage.
Meditation. This one is tough for me, but I highly recommend the work by Dan Harris on this subject. He became interested in happiness and meditation after having an on-air panic attack that millions witnessed. As a result, he became interested in the healing powers of meditation, writing a book and developing an app, both of which I’ve found incredibly helpful. It’s easy reading and he somehow manages to be both informed and self-deprecating.
Reading. I love to read, but need to be picky about the tone and subject matter of the book depending on my mood. Sometimes I want to learn, sometimes I want to laugh, sometimes I want to escape. If you need ideas for good books, check Pinterest or go to the GoodReads app to see what your friends recommend.
Talk to a friend. Most likely your friends have struggled with some issue in their life, maybe not infertility, but something that they needed to manage. It’s ok to share your challenges with them. Most are grateful that you are willing to open up to them. Your job, in return, is to cultivate your listening skills. This book by Celeste Headlee really helped me with this and I recommend it to all of my clients and friends.
I am happy to talk to you or your daughters about their fertility. Honored, actually. But some of you ask me what you can do, besides refer them to me. In this situation, you don’t have to be an infertility nurse to make a difference. Encourage them to develop inner strength. If you think they are struggling, ask them, as their Facebook posts aren’t always a reliable reflection of their inner psyche. Support them in the knowledge that it’s ok to allow external events to affect you, without defining you.
“A healer is not someone that you go to for healing. A healer is someone that triggers within you, your own ability to heal yourself.” –Unknown
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Cookie
Duration
Description
_mcid
1 year
This is a Mailchimp functionality cookie used to evaluate the UI/UX interaction with its platform
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Cookie
Duration
Description
_ga
1 year 1 month 4 days
Google Analytics sets this cookie to calculate visitor, session and campaign data and track site usage for the site's analytics report. The cookie stores information anonymously and assigns a randomly generated number to recognise unique visitors.
_ga_*
1 year 1 month 4 days
Google Analytics sets this cookie to store and count page views.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
Cookie
Duration
Description
VISITOR_INFO1_LIVE
6 months
YouTube sets this cookie to measure bandwidth, determining whether the user gets the new or old player interface.
VISITOR_PRIVACY_METADATA
6 months
YouTube sets this cookie to store the user's cookie consent state for the current domain.
YSC
session
Youtube sets this cookie to track the views of embedded videos on Youtube pages.
yt-remote-connected-devices
never
YouTube sets this cookie to store the user's video preferences using embedded YouTube videos.
yt-remote-device-id
never
YouTube sets this cookie to store the user's video preferences using embedded YouTube videos.
yt.innertube::nextId
never
YouTube sets this cookie to register a unique ID to store data on what videos from YouTube the user has seen.
yt.innertube::requests
never
YouTube sets this cookie to register a unique ID to store data on what videos from YouTube the user has seen.